

Introduction: Since 2017, several new therapies were approved by the United States (US) Food & Drug Administration (FDA) for the treatment of acute myeloid leukemia (AML), many of which target specific gene mutations. Enasidenib, a once-daily oral tablet, was approved by the FDA in August 2017 for patients with relapsed or refractory (RR) AML with an isocitrate dehydrogenase-2 (IDH2) mutation, which occurs in 8-19% of patients with AML. While efficacy was established in a phase 3 trial that demonstrated a complete remission (CR)/CR with partial hematologic recovery (CRh) rate of 23% and a median remission duration of 8.2 months, data outside the trial setting are lacking. This study aimed to assess real-world outcomes (i.e. response to therapy, survival, and rates of emergency department [ED] visits and hospitalizations) among a large cohort of patients with RR AML with IDH2 mutations treated with enasidenib, or other systemic therapies, in the first-line (1L) RR setting.
Methods: A retrospective, observational cohort study of patients with RR AML and IDH2 mutations treated with enasidenib between January 2018 and June 2019, or with another approved RR AML therapy (including cytotoxic chemotherapy, hypomethylating agent, targeted therapy, e.g. venetoclax) between January 2016 and July 2017 as 1L RR therapy, was conducted. Data were collected from patient medical records abstracted by 20 community oncologists across all geographic areas in the USA (30% Northeast, 20% Midwest, 25% South, 25% West). Patient characteristics, treatment patterns, physician-reported response to 1L RR therapy, ED visits, hospitalizations, and date of death were collected. Descriptive statistics were used to summarize patient characteristics and outcomes, and univariate comparisons were made by chi-square and t-tests. Median (95% confidence interval [CI]) progression-free survival (PFS) and overall survival (OS) from 1L RR therapy initiation were estimated by the Kaplan-Meier method, and adjusted risk (hazard ratio [HR] and 95% CI) of progression and death were estimated by multivariable Cox proportional hazard models to control for potential confounders.
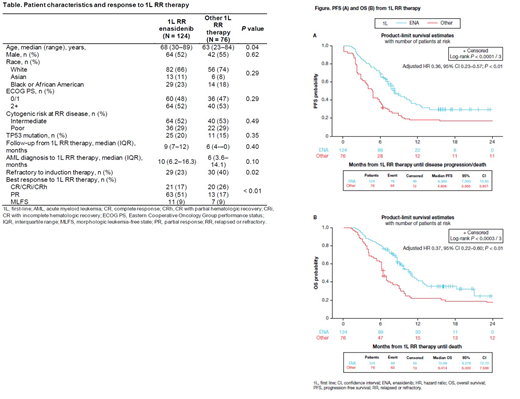
Results: Of the 124 patients treated with enasidenib and 76 control patients treated with another (non-enasidenib) 1L RR therapy for RR IDH2-mutated AML, 52% and 55% were male (P = 0.62), and median age at 1L RR therapy was 68 and 63 years (P = 0.04), respectively (Table). The proportion of patients with European Cooperative Oncology Group performance status (ECOG PS) 2+ (52% vs 53%) and poor cytogenetic risk (29% vs 29%) were similar among enasidenib and other 1L RR therapy patients, respectively (both P > 0.05). Approximately 23% of 1L RR enasidenib patients were refractory to induction therapy versus 40% of other 1L RR therapy patients (P = 0.02). CR/partial response/morphologic leukemia-free state rate was higher among patients treated with enasidenib versus other 1L RR therapies (77% vs 52%; P < 0.01). After a median follow-up of 9 and 6 months from 1L RR treatment among enasidenib and other 1L RR therapy patients, respectively, median PFS was 8.4 and 4.8 months (adjusted HR = 0.36, 95% CI 0.23-0.57; P < 0.01), and median OS was 11.0 and 6.4 months (adjusted HR = 0.37, 95% CI 0.22-0.60; P < 0.01), respectively (Figure). While rates of ED visits were similar across treatment groups (22% 1L RR enasidenib vs 18% other 1L RR therapy, P = 0.59), fewer 1L RR enasidenib patients were hospitalized during 1L RR therapy versus other 1L RR therapies (14% vs 46%, P < 0.01).
Conclusions: Results from this large real-world cohort study confirm the effectiveness of 1L RR enasidenib among patients with IDH2-mutated AML outside the trial setting and are similar to the pivotal phase 3 trial results. Superior response rates, PFS, and OS were observed in enasidenib-treated patients compared with other commonly used 1L RR therapies. Additionally, rates of hospitalizations were significantly lower among those treated with 1L RR enasidenib versus other 1L RR therapies. Further research is warranted to understand how and when physicians test for mutations and apply targeted therapies and how practicing physicians assess response to contemporary RR AML therapies in real-world clinical practice.
Klink:Cardinal Health: Current Employment, Current equity holder in publicly-traded company. Copher:Bristol Myers Squibb: Current Employment. Knoth:Bristol Myers Squibb: Current Employment. Marshall:Cardinal Health: Current Employment. Hou:Cardinal Health: Current Employment. Gajra:Cardinal Health: Current Employment. Tibes:Celgene/BMS: Consultancy, Honoraria.

